
Premature Ejaculation
What Is It?
This article is a repost which originally appeared on Harvard Health
Edited for content
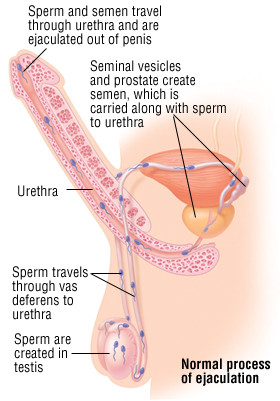
Premature ejaculation occurs when a man reaches orgasm and ejaculates too quickly and without control. In other words, ejaculation occurs before a man wants it to happen. It may occur before or after beginning foreplay or intercourse. Some men experience a lot of personal distress because of this condition.
As many as one in five men experience difficulty with uncontrolled or early ejaculation at some point in life. When premature ejaculation happens so frequently that it interferes with the sexual pleasure of a man or his partner, it becomes a medical problem.
Several factors may contribute to premature ejaculation. Psychological problems such as stress, depression and other factors that affect mental and emotional health can aggravate this condition. However, there is growing evidence that biological factors can make some men more prone to experience premature ejaculation.
Rarely, premature ejaculation can be caused by a specific physical problem, such as inflammation of the prostate gland or a spinal cord problem.
 |
Symptoms
The key symptoms of premature ejaculation include:
- Ejaculation that routinely occurs with little sexual stimulation and with little control
- Decreased sexual pleasure because of poor control over ejaculation
- Feelings of guilt, embarrassment or frustration
Diagnosis
Premature ejaculation is diagnosed based on typical symptoms. To understand your problem, your doctor will need to discuss your sexual history with you. Be frank and open. The more your doctor knows, the better he or she can help you.
If your sexual history fails to reveal significant mental or emotional factors that may contribute to premature ejaculation, your doctor may want to examine you. Your doctor may examine your prostate or do neurological tests (tests of your nervous system) to determine if there is a physical problem that could be causing premature ejaculation.
Expected Duration
Sometimes, premature ejaculation goes away on its own over weeks or months. Working to relieve stress or other psychological issues may help the situation to improve.
Other men have lasting difficulties with premature ejaculation, and require professional help. Some men respond to treatment promptly, while others struggle with this problem over a prolonged period. Effective treatment is available.
Prevention
There is no known way to prevent premature ejaculation. However, you should consider the following advice:
- Maintain a healthy attitude toward sex. If you experience feelings of anxiety, guilt or frustration about your sex life, consider seeking psychotherapy or sexual therapy.
- Keep in mind that anyone can experience sexual problems. If you experience premature ejaculation, try not to blame yourself or feel inadequate. Try speaking openly with your partner to avoid miscommunication.
Treatment
Behavioral therapy is one possible approach for treating premature ejaculation. Most commonly, the “squeeze technique” is used. If a man senses that he is about to experience premature orgasm, he interrupts sexual relations. Then the man or his partner squeezes the shaft of his penis between a thumb and two fingers. The man or his partner applies light pressure just below the head of the penis for about 20 seconds, lets go, and then sexual relations can be resumed. The technique can be repeated as often as necessary. When this technique is successful, it enables the man to learn to delay ejaculation with the squeeze, and eventually, to gain control over ejaculation without the squeeze. Behavioral therapy helps 60% to 90% of men with premature ejaculation. However, it requires the cooperation of both partners. Also, premature ejaculation often returns, and additional behavioral therapy may be needed.
Another possible treatment is prescription medication that helps to delay ejaculation. Delayed orgasm is a common side effect of certain drugs, particularly those used to treat depression. This is true even for men who are not depressed. When this type of medication is given to men who experience premature ejaculation, it can help to postpone orgasm for up to several minutes. Drugs used for this type of treatment include selective serotonin reuptake inhibitors (SSRIs), such as fluoxetine (Prozac), paroxetine (Paxil) or sertraline (Zoloft); and tricyclic antidepressants, such as clomipramine (Anafranil).
Some men with premature ejaculation may benefit from drugs called phosphodiesterase inhibitors, such as sildenafil (Viagra), vardenafil (Levitra), and tadalafil (Cialis). A phosphodiesterase inhibitor can be used alone or in combination with an SSRI. One drug should be started at a time, preferably at a low dose.
Some men with premature ejaculation also benefit from reducing the stimulation they experience during sex. A number of creams are available that can partially anesthetize (numb) the penis and reduce the stimulation that leads to orgasm. Another option is to use one or more condoms. However, these techniques may interfere with the pleasure experienced during sex.
When To Call a Professional
Speak with your doctor if you consistently ejaculate before you want to. Remember, one instance of premature ejaculation does not mean that you have a condition that requires treatment. Your doctor may refer you to a sex therapist if premature ejaculation is causing major problems in your sex life or personal relationships or if you would like to consider behavioral therapy.
Prognosis
Many men experience a brief period of premature ejaculation, then improve on their own. Even for men who require medical treatment, the outlook is usually good.


 I am 26 years old and I recently developed this mythical problem called Hard Flaccid.
I am 26 years old and I recently developed this mythical problem called Hard Flaccid. Almost 2 months ago, while I was having sex with my girlfriend, I started to lose my erection suddenly, after performing an intense Kegel, during a sex position that placed my penis at a downward angle (so, I did a “very weighted Kegel”).
Almost 2 months ago, while I was having sex with my girlfriend, I started to lose my erection suddenly, after performing an intense Kegel, during a sex position that placed my penis at a downward angle (so, I did a “very weighted Kegel”). – Now, I only have hard flaccid if I’m standing. A few times, I don’t even have it standing. It happens when I get up after doing Reverse Kegels for a few minutes (or sitting for a while in a more comfortable position) and continue to do Reverse Kegeling while I’m standing. This was impossible 1 month ago.
– Now, I only have hard flaccid if I’m standing. A few times, I don’t even have it standing. It happens when I get up after doing Reverse Kegels for a few minutes (or sitting for a while in a more comfortable position) and continue to do Reverse Kegeling while I’m standing. This was impossible 1 month ago.